| Listen Now | Category | series_hfilter |
|---|---|---|
In this episode, the whole team is back for a spirited round of “EMS Jeopardy.” Steve takes on the role of game show host as Dan and Holly face off, answering questions across categories like airway and breathing, cardiology and resuscitation, medical emergencies, trauma and shock, EMS protocols and safety, and basic pharmacology. Tune in for a fun and informative review of EMS topics at all difficulty levels, brought to life by the lively banter of some of the field’s most respected and well-known professionals.
References:
|  Medical Medical | medical |
EMS is notorious for the high stress, long hours, and repeated exposure to trauma that leave an alarming number of burned-out professionals in its wake. Whether you work for a private ambulance, fire department, or in a hospital setting, burnout is a real and pervasive threat to the well-being of any EMS provider. And, where burnout is often found, so is a toxic workplace. In this episode, Steve, Dan, and Holly talk about their experiences in toxic environments or around toxic individuals. They discuss how easy it is to become part of the toxic culture, and why that makes it crucial to recognize associated patterns of thoughts and behavior and rise above them. The team then walks through steps to prevent becoming entrenched in the thoughts and behaviors that lend themselves to toxicity. This episode provides an opportunity to reflect both on one’s environment and to look inward to examine if there are aspects of toxicity that have crept into our thoughts and practices. It also gives helpful tools to self-correct to preserve our mental health and support and improve our department’s culture.
References:
|  Operations Operations | operations |
In this episode, Steve, Dan, and Holly are back in the studio as Holly leads the team through an in-depth discussion on the trauma death triad (diamond). They discuss each component – hypothermia, acidosis, coagulation – and that tricky final component that plays a role in all three, calcium. Holly provides a scientific breakdown of each component, and then the team discusses the practical implications of each component in the “real-life” management of a trauma patient in the field. Holly also touches on some longer-term implications of trauma management for those providers who end up on scene with a patient for longer than they bargained for or who provide an interfacility transfer for a patient a few days after their initial incident. This episode provides helpful insight for all providers in both the initial and ongoing assessments of any patient who has experienced a massive trauma, and what we can do in the field to mitigate mortality and positively impact their overall outcomes. References
See Holly’s slides below! |  Trauma Trauma | trauma |
In this episode, Steve, Dan, and Holly are joined by guest Matt Shamrell, a burn unit ICU nurse. Matt discusses treatment processes for burn patients, including fluid resuscitation, pain management, and wound care. Matt answers questions about risk factors for, and the in-hospital management of, compartment syndrome as well as the potential for severe and life-threatening infections in burn patients. The team discusses how EMS providers can best treat burn patients to ensure the transition of care from pre-hospital to in-hospital is as seamless as possible. | Trauma | trauma |
Steve and Dan co-host their first show without Holly as they welcome special guest Eric Jaeger. Eric is an RSI Paramedic and Attorney from New Hampshire who leads the discussion on best practices for physical restraint and chemical sedation and the legal ramifications these interventions carry. Eric shares his knowledge of the tragic circumstances surrounding George Floyd and Elijah McClain’s deaths and discusses improvements to consider when it comes to protocols and guidelines for these procedures. | Operations | operations |
In today’s episode, Steve, Dan, and Holly have the opportunity to discuss an interesting MCI call with guest, Firefighter/Paramedic Kyle Snider. At the time of the incident, Kyle was a new paramedic graduate with wilderness medicine training who was working in a rural department with limited resources. Kyle discusses the call from the point of dispatch to call completion and reviews what he felt went well and what he would have changed. This episode gives the team a chance to discuss how we often leave chaotic scenes feeling overwhelmed and discouraged; however, reviewing the call with others in the field can be helpful to see where we performed well and where or what we could do to make improvements if faced with a similar call in the future. When discussing this call, we see how Kyle managed as the PIC and only paid medic while ensuring all patients received care. He then took what he learned from this call to help make personal and departmental improvements moving forward. | Trauma | trauma |
It is no secret that we, as a nation, are experiencing extreme implications of opioid abuse. In this episode, Holly talks about a new program she is helping head, whose goal is to provide treatment to patients suffering from opioid addiction. This cutting-edge program utilizes a medication called buprenorphine to initiate treatment in the field and provide ongoing care for willing patients. While there is still much to learn, Holly discusses the research behind the foundation of this program, its successes thus far, and some learning points. The team discusses how this information is helping shape the current program and providing crucial data for future programs. This episode sheds light on current opioid abuse and overdose statistics, discussion around the steps of behavioral change, and relevant data on what treatment is proving most effective for individuals suffering from opioid addiction. Show Notes:
References:
| Medical | medical |
In this follow-up episode, Bruce and the team continue discussing ventilation and airway management. This episode goes into greater depth on how ETCO2 can be used to manage an array of patients effectively and how a thorough understanding and monitoring of end-tidal during a resuscitation attempt can help ensure a patient remains neurologically intact, assuming ROSC is achieved. Bruce covers case studies on this topic, and the team has the opportunity to look at the “oscillations” in end-tidal and how they provide vital information on the efficacy of CPR and PPVs. This episode provides unique insight and information on the delivery of effective ventilations and how to best use the tools in our toolbox to ensure our patients receive the highest possible level of care. This episode highlights the central theme of part 1: that airway management should not be lightly handed over to the least experienced provider; instead, thorough training should be provided to all members of a crew to ensure all are competent and understand the weight and importance of the delivery of effective ventilations to not only the management of the patient while they are in crisis, but to their longevity following the incident. Below are graphics and their descriptions provided by Bruce to help understand concepts discussed in the course.
This example shows “Oscillations, 30:2 Ventilations. This patient is intubated (Patent Airway). Tidal Volume is excellent, and compressions look high quality. You can see it all play out. Also, notice that in the 30:2, the first end-tidal waveform is shortened. That is because we are trying to give two really fast breaths, so we interrupt the first breath out with an immediate 2nd breath in, giving it a shortened waveform. This is trained at TVFR to give your two breaths and then look for a shortened waveform, and the 2nd breath has the compressions. Appreciate how consistently our variables work together, and the end-tidal is not wavering or all over the place.” – Bruce Opsal
The above example “Is a crew that gave the bonus breaths that I discussed in the podcast. Rhythm Change (Sinus Bradycardia), not perfusing, and the end-tidal drastically is dropping breath by breath. You might think, if I give 4 stacked breaths, wouldn’t that lower the end-tidal, and the answer is no. You will not have a drastic change as that, where the first breath is around 50 and by their 5th breath, it’s at 20. I would argue that it will just outright sustain if the heart is perfusing. A student contested this, so I just had him put on an end-tidal and a monitor and watched him dry to drop his capnometry even one point from 1 – 5 breaths, and he couldn’t do it.” – Bruce Opsal
|  Airway Airway | airway |
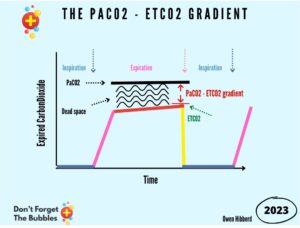
In this episode, Steve, Dan, and Holly talk with Bruce Opsal, a long-time firefighter and paramedic who has spent years leading training programs centered on effective airway management and ventilation. Bruce first emphasizes the importance of airway management in any patient, especially those in cardiac arrest. The team talks about how the previous line of thought was to assign the airway to the least experienced provider and then forget about it. However, this is evolving in pre-hospital management as we better understand the importance of careful and attentive airway management. Bruce then introduces his 6-step process for confirming effective ventilations, and through this discussion, providers of all levels can glean helpful tools for effective airway management and successful delivery of ventilations. The team spends the most time on one step that is not often well understood, which is end-tidal (ETCO2). Throughout their discussion, Bruce and the team go through what end-tidal is measuring, how it can confirm effective PPVs and/or airway placement, and how it can be used to manage a patient successfully during cardiac arrest. This episode allows listeners to challenge the current thought processes around out-of-hospital airway management and gives a new perspective on effectively managing an airway. Below is a graphic and description provided by Bruce that will help the listener understand some of the concepts discussed in this course.
“[This] is a nice visual I found […] I like seeing the EtCo2 line and its relationship to CO2 in the blood. This helped me get to my soup analogy.” – Bruce Opsal | Airway | airway |
Dr. Selbak joins Steve, Dan, and Holly to discuss a few unique case studies. The episode begins with Steve walking the team through a call that raises many questions for his crew. As the case is discussed, the listener is encouraged to critically consider the patient’s history, symptoms, presentation, and additional lab values as they are given. At the same time, Dr. Ramsay discusses his process for assessing and managing this patient and ultimately comes to a diagnosis. The second half of this episode provides an overview of hyperkalemia – what it is, how it happens, how it often presents, and how it may be stabilized in the field and definitively treated in the hospital setting. Field providers do not often understand hyperkalemia and its field treatment, so the team breaks down the etiology of hyper-k and the mechanisms of action for the classic medications used to treat it in the field. The listener also gets insight into how these patients are managed in the hospital in the short and long term, which helps paint a complete picture of the hyper-k patient. This episode demonstrates the importance of history gathering and provides a deeper insight into lab values and how they are used to diagnose patients with less obvious disease processes. Listeners should walk away feeling better equipped to identify both endocrine and electrolyte imbalances in patients with unique presentations. | Medical | medical |
In this episode, Steve presents two trauma case studies for the group to discuss. While patient care in both of these calls went well, and these scenarios provide an overview of successful extrication and patient management following both an MVA and significant blunt force trauma, the distinguishing factor in each is a particular element that caught Steve “off guard” and forced him to revisit the call days or weeks later. As first responders, we often arrive on scenes that we assume will be “routine” or similar to calls we have been to before; however, it is essential to understand that sometimes there are elements of a call that, while on scene, may not affect our patient care or ability to perform, but later they stick with us and prevent us from adequately processing the call. The element that sticks or “catches us off guard” will vary, but the result is often the same…the memory refuses to file itself into our mental Rolodex of calls properly. It is like a page of a book that has folded and torn, catching on the pages around it and preventing the book from closing properly. For these calls, we hope to recognize these “sticking points” and seek help from a trusted mental health professional to prevent these points from gumming up the surrounding mental space and preventing us from processing all incoming information and future calls. This episode provides an interesting insight into trauma patient assessment, management, and transport. However, it also emphasizes the work we, as healthcare providers and first responders, must do to maintain pique mental health and continue to provide a high level of care to patients in unpredictable and ever-changing scenarios. | Trauma | trauma |
In today’s episode, the team talks with Daniel Sundahl, a 20-year Firefighter/Paramedic, and artist. Daniel discusses how his experiences navigating PTSD led him to create powerful artwork, which is now helping open the conversation around mental health for first responders. For decades, mental health care was neglected for those working in the field, meaning responders were repeatedly exposed to traumatic events with little (if any) time to process what they saw, heard, treated, and experienced. While stigmas are still attached to seeking care for mental health, the concept that only the weak need help is slowly being dismantled. Therefore, the team takes the time to broach this sensitive subject with the hopes of helping first responders across the country, continent, and world seek help and care while recognizing they are not alone. This episode delves into the evolution of mental health care with expanding research around mental health and traumas. It also emphasizes the value of those with years of experience using their history in the field to build a foundation of support and care for current and future first responders. If you or someone you know is in crisis or having thoughts of suicide, please call 988 (U.S.) or go to https://988lifeline.org/. If you want to view Daniel’s artwork, read more about his story, or see where his artwork will be on display, visit https://www.dansunphotos.com/. | Medical | medical |
In this episode, Steve, Dan, Holly, and Dr. Selbak review a few of their calls involving aortic dissections. Because aortic dissection is a relatively uncommon disease process, and many severe cases never make it to the hospital, reviewing these cases provides a unique opportunity for the listener to gather abundant knowledge in one sitting that may otherwise take years to gather in the field. The team also discusses how patient presentation, vital signs, and history gathering can point a provider towards aortic dissection over other cardiac or pulmonary conditions and how a few relatively simple tests in the ER can help confirm a field provider’s suspicions. The goal of this episode is to encourage listeners to be on high alert for a few key phrases and to be cautious about falling into the classic trap of overlooking a patient simply because their signs and symptoms may not be glaringly obvious or particularly alarming. We all know that two patients with the same etiology can present drastically differently, and this podcast not only provides a few clear examples of this but also sheds light on why that might occur. |  Cardiac Cardiac | cardiac |
In this episode, Steve, Dan, and Holly talk with Dr. Ramsey Selbak about the increasing prevalence of violence in healthcare. They each take a turn providing examples of dangerous situations they’ve been involved in, how they handled them, and how they have adjusted their tactics as providers since. This episode introduces a much-needed conversation about provider safety in healthcare and how it has long been neglected. The team touches on why violent incidents seem to be more commonplace, why they often go unreported, and the lack of debriefing many EMS providers have following these events. The team goes on to explore how a lack of training on entering unsafe scenes often puts providers at risk, and how much of this is because, historically, EMS providers did not enter unsafe situations without law enforcement. However, this seems to be changing, and EMS providers often have to call for law enforcement after the situation has already devolved. This episode forces the listener to reflect on their own experiences and consider steps each of us may need to take to keep ourselves, our patients, our crews, and future EMS providers safe in an ever-changing field. | Operations | operations |
In this episode, the team discusses specific ways efficiency can be improved in the field of EMS. Steve explains how his department has utilized a “pit crew” model and is blazing a trail for a “heads-up” approach to cardiac arrest response following incredible outcomes discovered by the Rialto (CA) Fire Department. Dan and Holly talk with Steve through the newly implemented 10-step checklist and how it has the potential to revolutionize cardiac arrest response. The team segues this conversation to the benefits of checklists on most EMS calls. They discuss how checklists can improve communication, prevent missed steps, and maintain organization on most scenes. Steve also brings up a common hang-up in EMS: the yard sale. How many times has a vital piece of equipment been lost in the debris of a chaotic call? Most have experienced this, and more than once. Steve and Holly mention some tips and tricks to prevent the classic “yard sale” and maintain equipment organization on scene, which can prevent items from being lost, helps with the continuity of the call and makes clean-up after the call much more manageable. This episode also calls EMS providers to think more critically about the “whys” of our emergency response. Can you move your department forward by being on top of new research and data? Or perhaps be bold enough to add visual aids like checklists and algorithms to our emergency response, overcoming the stigma that an experienced provider shouldn’t need help remembering critical steps? We encourage you to listen to this podcast considering the question, “How can I advocate for change that may improve patient outcomes in my department?”. | Operations | operations |
In this episode, Steve, Dan, and Holly have the opportunity to chat with Dr. Selbak in the studio. Dr. Selbak introduces a compelling case he came across while working in the emergency department. The group asks questions about the patient’s current condition and past medical history while discussing how they would likely treat the patient based on the provided information. Dr. Selbak talks with the team about more advanced in-hospital diagnostic techniques he and his team utilized to diagnose this patient and how it drastically altered their course of treatment. The team discusses ways field providers can employ some of these techniques and analyzes how we, in the field, can be on the lookout for some of these case outliers to better diagnose and treat our patients. As you listen, you will glean some incredibly helpful wisdom and insight into how we can best prepare our patients and the hospital staff for our arrival and paint a full diagnostic picture for the patient hand-off. | Cardiac | cardiac |
In this episode, Steve, Dan, and Holly discuss their experiences with OB calls, specifically field deliveries, that were outside a typical “textbook” experience. They dive into the aspects of the scene, patient, transport, and crew to discuss what made their experiences stand out. Each provider will also take the time to address a unique OB emergency related to the patient in their story or that they have experienced and how they treated that patient to benefit both mom and baby. OB calls, specifically those in which deliveries are imminent, are low frequency with the potential to be very high risk. So the team discusses how they felt going into the call, what they did that helped set them up for success, and what about the scene created a roadblock as they attempted to provide the best possible patient care. While each patient discussed delivered otherwise healthy babies, listener discretion is advised as these stories involve less-than-ideal scenarios with challenges in both patient care and scene management. |  OB/GYN OB/GYN | obgyn |
In this special episode, we celebrate our co-host, Dan Livengood, on his retirement after 27 years in the fire and EMS service. Dan is one of the most selfless and caring people you’d ever hope to have show up at your door during your time of need. We learn from his co-workers just how much fun it was to work with Dan and what life in the firehouse with him was like. | Medical | operations |
In this episode, Steve, Dan, and Holly discuss EMS education with Adam Culbertson, a current educator in North Carolina. The team has the opportunity to ask Adam about EMS education and how it is changing, as well as some trends we can expect to see in the coming years. Adam explores what has worked really well in his own education, as well a with his students, and what does not seem to be benefiting them. He goes on to explain how he and his fellow educators are trying to use that knowledge and understanding to enhance curriculum and classroom settings for incoming students and providers. This episode highlights current struggles in EMS and how better preparation in the classroom can lead to providers who are well-equipped to be lifelong learners. Also highlighted are disparities in mental health, both in the treatment of patients, as well as in caring for ourselves and our coworkers. Overall, this episode helps sets the stage for the foundational evolution taking place in EMS. | Operations | operations |
In this episode, Steve, Dan, and Holly are joined by Dr. Ramsey Selbak, EMTprep’s Physician Advisor. Dr. Ramsey discusses his background in emergency medicine as well as his experience and relationship with field providers. The team then delves into an age old rut into which many EMS providers fall – chasing numbers. What do we mean by this? Trying to correct specific lab values or vitals without taking into account the entirety patient. What do they look like? Why might this vital or value be skewed? How long did it take the patient to get to where they are now? And, of course, is the patient stable as they sit? Dr. Ramsey provides a couple brief examples of times where seemingly critical patients remain stable with limited intervention in the ED, which implores the crew to discuss the role of EMS providers in the field, and re-evaluate their responsibility to “fix” or “reverse” patients with advanced disease processes. | Medical | medical |
In this episode, Steve, Dan, and Holly discuss calls that are not “black and white,” and have forced them to think outside the box. Steve provides Dan and Holly with a case he encountered and has them walk through their decision-making. He then reflects on how he and his crew responded to the scenario. Holly reviews a call she had that presented a variety of challenges and forced her to work in the “gray zone” and defend the clinical decisions she made to her agency and receiving hospital. The team closes by reviewing the importance of critical thinking and its application in the world of emergency medicine. | Medical | medical |
Steve, Dan, and Holly are back in the studio after a 6-month hiatus. The team reviews disaster medicine, how to get in the door, and what to expect on deployments. Dan Livengood is interviewed and discusses his multiple deployments that started in 2001 in El Salvador up to his most recent deployment to Ukraine. To help Ukraine, visit:
| Operations | operations |
Steve is back in the studio to give you a quick update on our friend and guest, Debbie Bailey. Steve gives a timeline for when the trio will be back in the studio again to record the next episodes of the show. | Medical | medical |
Steve, Dan, and Holly bring special guest Debbie Bailey on the show to discuss the process of dying and death itself. The trio listen as Debbie describes her battle with a terminal illness and what her recommendations are for EMS providers who are called to treat those in their final days and moments. | Medical | medical |
Steve, Dan, and Holly bring in Dr. Ramsey Selbak to discuss Ketamine use from an ER Physician’s perspective. In addition to some case reviews, key aspects of Ketamine dosing, indications, and side effects are discussed. | Medical | medical |
Steve, Dan, and Holly bring Nate and Andrea from the Guardian Group into the studio to discuss Sex Trafficking Awareness. As EMS providers, Nate and Andrea walk listeners through what to look for on scene, best practices when you find evidence of trafficking, and how to protect your loved ones at home. | Operations | operations |
Steve, Dan, and Holly discuss the background and use of Ketamine in EMS. The trio interviews their guest, Oregon Firefighter/Paramedic Isaiah Burkhart, an Army Ranger veteran, about his experience with Ketamine personally and professionally. Various calls are discussed outlining what went well and what could have gone better when it comes to chemical restraint. Various doses and indications for the drug are discussed along with what the future of Ketamine use could look like in depression and psychotherapy treatment modalities. | Medical | medical |
Steve, Dan, and Holly are joined by Dr. Ed Racht to discuss humor and its role in EMS. Gallows humor is discussed as well as the concept of looking at humor as a different language for EMS providers. Dr. Racht reviews when to know you’ve crossed the line and how to test your humor out with your co-workers, friends, and family if you’re unsure if it will be received well. | Operations | operations |
Steve, Dan, and Holly are joined with their colleague Chad who works full time in human trafficking in the Portland area. Chad describes his work, defines trafficking for listeners, and outlines what EMS providers can do when their “spidey senses” are going off. Mental health awareness is discussed when it comes to first responders who are constantly faced with gut-wrenching calls and cases. Steve and Dan discuss calls where they felt something was off and took various actions which may have helped get their patients the resources they needed. | Operations | operations |
Steve, Dan, and Holly discuss the fundamental differences and pros and cons between private ambulance EMS and Fire-Based EMS. The trio is joined by two Firefighter Paramedics from Washington State – Eric Chamberlain and Jeff Wright, who have a unique outlook on EMS compared to the average of their peers. |  Pediatrics Pediatrics | operations |
Steve, Dan, and Holly return to discuss the generational gaps in EMS and the workforce in general. The trio talks about the common stereotypes and strengths of Baby Boomers, Gen X, Xennials, Millenials, and Gen Z. The trio details their own personal experiences working with people across all generations and how those differences can make work fun. The differences between millennials and the other generations in the workplace are examined. | Operations | operations |
Steve, Dan, and Holly are back after an extended hiatus due to COVID-19. Listen as the trio discuss how COVID has impacted their lives both professionally and personally. Compassion fatigue and the impact of the Coronavirus on healthcare workers across multiple disciplines are discussed. Steve discusses one of his recent COVID-related cardiac arrest calls and the changes EMS is facing in the waking of the pandemic. | Medical | medical |
Steve, Dan, and Holly return to discuss the pathway to a successful internship. The trio talks about how formative internship is for students and begins answering questions submitted by prospective students. The importance of studying protocols is highlighted; many agencies require that new interns be competent with their specific protocol. If possible, seek internships outside of areas that are familiar. Agencies with high call volumes allow for ample opportunities to practice a variety of medical skills in a short amount of time. The trio details the stress of the first day of internship, and what students can expect. Adaptation is key; different agencies operate differently and have their own unique challenges. Steve reminisces about his internship, and how the system he worked in operated. Holly, Dan, and Steve each give their number one tip for success during the internship. The importance of attitude is discussed, as well as being open to learning from professionals with years of experience. Steve reviews how to regroup after being stumped on a call. The trio talks about favorite qualities in their respective preceptors. Qualities that are important for emergency medical providers to cultivate are debated. To wrap up the podcast, the trio discusses common issues paramedics can run into, and the importance of self-care. | Operations | operations |
Dan, Holly, and Steve return to discuss resiliency and its importance in emergency medical services. Dan and Holly open by highlighting their attendance at the Train the Trainer course for the FBI Officer Resiliency course. The definition of resiliency is debated, and the trio talks about how each individual will reflect resiliency differently. Steve recaps how his parents instilled resiliency in him from a young age, through de-stigmatizing psychological counseling. Holly and Dan further detail the organizational components of their course, and its emphasis on teaching resiliency early. Story-telling was focused on in the course, as a way to help everyone open up. Holly and Dan review the science behind dealing with stress and building resiliency. One main focus of the course was ABC: activating event, breathe, and then dealing with the consequences. Understanding how the human brain and body react to stress is a key element in dealing with the effects of that stress in all environments. Holly and Dan further discuss how identifying values helped them learn more about themselves. Setting goals that correspond with one’s values will make reaching those goals easier. The trio calls Scott, a fire chief from Texas, who recounts a story about finding peace and appreciating our individual journeys. The group highlights the importance of practicing gratitude. The trio wrap up the podcast reflecting on the material discussed in the FBI Officer Resiliency course, and how they apply the philosophies outlined into their own lives. | Medical | medical |
Steve, Dan, and Holly are joined by special guest, Dr. Brenda Tillman of Readiness Group, to discuss how we as first responders can deal with chronic stress. In today’s world of Covid, natural disasters, social unrest, and political division, it’s hard to maintain our sanity when you throw in a stressful job on top of it. Dr. Tillman reviews ways we can practice good self-care to stay sane and improve our resilience. | Operations | operations |
In this episode, Steve, Dan, and Holly discuss lung sounds, their treatment modalities, and common misconceptions. Steve leads a Lung Sound recognition game while Dan and Holly square off to see who’s the best. After listening to the lung sound, they then discuss the correct sound by reviewing the textbook definition of it and the treatment options for it in the field.
| Airway | airway |
In this episode, Steve, Dan, and Holly talk about cardiac arrest response with the EMS coordinator at Rialto Fire, Joe Powell. After looking at Rialto Fire departments stats, Joe realized they had to do something different. At Rialto Fire, they have committed to the ‘wheel of survival’ which is a regularly evolving set of steps designed to maximize the interventions of EMS personnel with their patients who are experiencing cardiac arrest. Their stats on cardiac survivability have improved significantly since implementing this and they have multiple studies published in JEMS.
Wheel of Survival: Rialto_Cardiac_Survivability_Toolbox | Cardiac | cardiac |
Steve, Dan, and Holly introduce Scotty Bolleter, one of the co-inventors of the EZ-IO. Scotty details how he got started in EMS, and what led him to help create the EZ-IO. Scotty discusses his time as a flight paramedic, and how his time spent training in hospitals pushed him into EMS business ventures. Steve touches on his business ventures in EMS. Scotty walks the trio through his team’s process of modifying older devices to create their version of the EZ-IO. Scotty talks about his inter-disciplinary team of physicians, engineers, and others. The correct process of placing a humeral IO is discussed, from positioning the patient to proper placement for insertion. The process of IO flow is explained. Scotty discusses possible complications if an IO is placed wrong. Scotty discusses the use of the distal femur IO placement in cardiac arrest at his department. IO placement in the femur versus the humerus or the tibia is compared. Pediatric IO placement is reviewed. Scotty highlights the open IO, and when it is indicated. Correct IO placement is recapped, and Scotty touches on why EMS providers should not bury an IO needle into the bone. Steve reviews a call on a patient in status seizure where an IO is used for access. | Medical | medical |
Steve, Dan, and Holly introduce their guest speaker, Kari, a respiratory therapist/paramedic from Washington. Kari discusses the endotracheal tube and the importance of having a correctly sized and placed tube. Kari highlights how critical it is to understand the disease processes that resulted in the patient being intubated. Ventilation and oxygenation issues are reviewed, along with the importance of PEEP in intubated patients. Kari talks about PEEP in intubated patients with asthma or COPD, as well as variations in tidal volume settings for various disease processes. The group discusses minute volume, and how a patient’s minute volume is calculated on the ventilator. Kari discusses her process of titrating ventilator settings to meet a CO2 goal. Do no harm is reviewed in relation to mechanical ventilation, and the consequences of a patient working against the ventilator are discussed. Assist control (AC) and synchronous intermittent mandatory ventilation (SIMV) modes are compared. Kari details what modes she prefers for specific patient presentations and disease processes. The group discusses volume and pressure control, and review a trauma scenario where the patient is intubated. Peak inspiratory pressure and peak alveolar pressure are reviewed, along with what abnormal values can indicate. The importance of driving pressure is highlighted. The PF ratio is discussed, along with the importance of weaning patients off of 100% FiO2. The group ends on discussing appropriate IE ratios in obstructive patients. The flow rate in both volume and pressure control is reviewed, as well as the effect of flow rate on a patient in both volume and pressure control settings. Another scenario is discussed, a COPD patient that has been intubated. Kari walks through troubleshooting tactics for ventilators and potential fixes for common issues with mechanical ventilators. | Airway | airway |
Steve, Dan, and Holly introduce themselves, and today’s focus, trauma. Steve reviews his educational background, and how his university set him up for success in paramedicine. He then transitions into his craziest trauma call, dispatched a potential stabbing. Walking into the scene, Steve sees his patient, a 20-something-year-old who has been stabbed two times in the chest and once left arm. The crew bandages the superficial bleeding chest laceration, and places and tourniquet on the left arm laceration. When the patient loses consciousness, Steve has to act quickly to handle a tension pneumothorax. Steve, Dan, and Holly discuss the sequence of assessing a trauma patient. The physiological process of a tension pneumothorax is reviewed. The trio discusses what signs and symptoms indicate the need for a needle decompression in the field. Proper placement of the needle during a chest decompression is outlined. Holly sheds some light on what occurs in the hospital after a patient is dropped off with a decompressed tension pneumothorax. Dan details his craziest trauma call, which began on the way to a public education event. Enroute, Dan and his partner receive a call, a GSW to the face. The team performs a surgical cricothyroidotomy on scene in order to establish a patent airway. Dan discusses his thought process on the call and outlines his preferred method of performing a surgical cricothyroidotomy. Dan, Holly, and Steve review surgical cricothyroidotomy. Holly talks about her trauma call, which began as a search and assist on a mountain top. After assistance from a local volunteer firefighter, Holly and her partner arrive on scene to a single-vehicle MVC off the side of a cliffside. Five patients are present, three alive and two deceased. Holly describes the scene, and discusses challenges to care. | Trauma | trauma |
Steve, Holly, and Dan are back with Dr. Brenda Tillman and Ben Wescott in part two of their PTSI series. Dr. Tillman emphasizes how important it is for senior providers to encourage open discussions on mental health. Ben shares his insight on how providers can challenge the stigma of discussing mental health. Ben shares his story and highlights his path to healing. Dr. Tillman and Ben discuss peer support groups and educating departments on PTSI and PTSD symptoms and prevention. Steve, Holly, and Dan field questions to Dr. Tillman and Ben. Dr. Tillman outlines ways departments can implement peer support groups. | Medical | medical |
Steve, Dan, and Holly introduce Dr. Brenda Tillman and Ben Wescott in their seventh podcast. Dr. Tillman discusses her experience as a clinician, and Ben introduces himself. Dr. Tillman details the difference between PTSD and PTSI, and why those differences are important when diagnosing first responders. Counseling programs for first responders are overviewed, as well as the training process for counselors counseling first responders. Dr. Tillman reviews the process of EMDR and why it is effective for improving symptoms of PTSI and PTSD. The physiological effects of PTSD and PTSI are detailed. Steve talks about his experience with EMDR. Coping mechanisms in first responders are debated. Dr. Tillman talks about the importance of normalizing the symptoms of PTSI in first responders, and why peer support group and counseling is so essential. | Medical | medical |
Steve, Holly, and Dan begin their sixth podcast discussing the difference between PTSD and PTSI. Steve touches on his journey with PTSI. The initial triggering call is reviewed, and Steve details the emotional and physiological symptoms he dealt with. Steve talks about his experience with counseling. The trio overview common emotional and physiological symptoms of PTSI, as well as behaviors that can manifest from it. They describe the difference between debriefing and defusing. The importance of emergency medical responders taking care of themselves is highlighted. | Medical | medical |
Steve, Dan, and Holly begin their fifth podcast with a case study on a motorcycle accident. Dan describes the logistics of the call and initial patient presentation. Mistakes made during rapid sequence intubation are discussed. The trio talks about the evolution of airway management procedures, such as the process of intubating patients and pre-oxygenation. Dan discusses his checklist for successful rapid sequence intubation. Steve reviews his checklist, along with his triggers for backup airway placement and cricothyrotomy. Holly recaps a call where she decided against intubation and describes her thought process. | Airway | airway |
Steve outlines his “craziest” cardiac call for Holly and Dan, which was dispatched as a person down. He discusses logistical issues affecting patient care, and how those issues were addressed. Steve, Dan, and Holly review the call and talk about lessons learned. Dan breaks down his “crazy” cardiac call for Holly and Steve, which was dispatched as a cardiac arrest. The three review patient care rendered prior to arrival and patient care performed by Dan and his team. Lessons learned are discussed. | Cardiac | cardiac |
Holly talks about her background as a paramedic and flight nurse. Dan discusses certifications he obtained to become a flight paramedic. Holly discusses her path to become a flight nurse. The trio outlines similarities in protocols for flying a critical patient in the field. Holly touches on the importance of flying patients with time-sensitive presentations, be it medical or trauma-related. Dan and Holly describe their typical day, and what their crew and individual agencies look like. The two talk logistics when responding to a scene call in the helicopter. The influence of weather on flying is discussed, and Holly goes over the limitations of IFR and VFR aircraft. Ground contact protocol and communication between ground units and the flight team are overviewed. Steve reviews a call from his agency and fields Holly and Dan some questions regarding logistics and patient care. | Operations | operations |
In their second podcast, Dan and Steve discuss what their individual departments have done in response to COVID-19. Current statistics regarding the novel coronavirus are reviewed. Dan walks through what a call at his agency looks like in the midst of the COVID-19 pandemic. Steve touches on how COVID-19 has changed how departments respond to calls, as well as the mindset of medical providers on scene, exposure protocols, and PPE requirements. Steve discusses a call where proper PPE prevented him from having a life-threatening exposure. Dan outlines a breathing problem call at a care facility and the process of intubating a patient in respiratory failure. Dan details his decision to withhold intubation on a rapidly declining patient, and what backup airway he prefers to use in lieu of an ET tube. Steve and Dan talk about quarantine procedures for their agencies following exposure to COVID-19. | Medical | medical |
In their very first podcast, Dan and Steve introduce themselves and talk about their experience as medical professionals. The process of earning continuing education credit by listening to EMTpro podcasts is explained. Dan reviews two cases from his career, while Steve helps break down each case. The first case Dan reviews is a sick person call in a skilled nursing home. Dan discusses how unconscious bias influenced his initial resource management decisions before even arriving on scene. Scene assessment of the nursing facility is performed, along with the primary assessment of the patient and the first treatment decision. Dan attempts to stabilize the patient prior to hospital arrival. Dan and Steve talk about mistakes made and what could have been done differently. In the second case review, Dan is dispatched to a trauma scene call in the helicopter. The differences in airway management at the time of the call are discussed. Dan talks about how his attitude caused problems receiving information from resources on scene, and the consequences that resulted. Mistakes made were discussed, and important trauma assessment skills were highlighted. | Airway | airway |